

Anatomic shoulder replacement surgery is a procedure used to replace the damaged ball and socket of the shoulder joint with a conventional anatomic implant. This surgical approach is designed to closely replicate the shoulder’s natural structure and biomechanics. It may be recommended when conditions such as advanced shoulder arthritis or severe joint degeneration are causing persistent pain, stiffness, or loss of movement that has not improved with appropriate non-surgical care.
Unlike reverse shoulder replacement, an anatomic shoulder replacement preserves the normal orientation of the shoulder joint. The humeral head (ball) is replaced with a smooth metal implant, and the glenoid (socket) is resurfaced with a polyethylene component. This design relies both on a healthy, functioning rotator cuff to control movement and provide stability, as well as well preserved bone stock on the socket side (glenoid) to provide a foundation for the implant.
The shoulder is a ball-and-socket joint formed by the humeral head, which is the rounded top of the upper arm bone, and the glenoid, which is the shallow socket of the shoulder blade. In a healthy shoulder, these joint surfaces are covered with smooth cartilage that allows the joint to move freely and without friction. When cartilage becomes damaged or worn away, the joint surfaces become rough and irregular, and this condition is arthritis. This leads to inflammation, pain, loss of movement, and difficulty performing everyday tasks such as reaching, dressing, lifting, or sleeping comfortably.
The procedure is intended to improve joint comfort and movement, although individual outcomes vary depending on factors such as overall shoulder condition, muscle function, bone quality, and rehabilitation participation. Dr Richard Dallalana performs a thorough assessment to determine whether an anatomic shoulder replacement is suitable and to ensure that surgical planning is tailored to each patient’s anatomy, lifestyle, and functional goals.
One of the most common symptoms of advanced shoulder arthritis is deep, aching pain within the shoulder joint. This pain is often worse with movement, particularly activities that involve lifting the arm overhead, reaching behind the back, or carrying objects. As arthritis progresses, pain may become more constant and may occur even during light activities or at rest.
Anatomic shoulder replacement surgery is most commonly performed to treat conditions that cause significant damage to the shoulder joint surfaces while the rotator cuff tendons remain functional. Because this procedure relies on the rotator cuff muscles to control and stabilise the joint, careful patient selection is important to support optimal outcomes.
Several shoulder conditions may lead to joint damage severe enough to require anatomic shoulder replacement:
Arthritis can develop following previous shoulder injuries, including fractures, dislocations, or ligament injuries. Even when initial injuries heal, damage to cartilage or changes in joint alignment may lead to gradual joint degeneration and long-term pain. Arthritis is very common after many years of playing collision sports.
Inflammatory joint conditions such as rheumatoid arthritis can affect the shoulder joint by causing chronic inflammation of the joint lining. Over time, this inflammation may damage cartilage and surrounding structures, leading to joint destruction and functional limitation.
Avascular necrosis occurs when the blood supply to the head of the upper arm bone becomes disrupted, causing the bone to weaken and collapse. As the joint surface deteriorates, pain and stiffness typically develop, and joint replacement may be considered in advanced cases.
The success of anatomic shoulder replacement relies heavily on a functioning rotator cuff. These muscles stabilise the joint replacement. If the rotator cuff is significantly damaged or irreparable, alternative surgical options, such as reverse shoulder replacement, may be more appropriate.

Although anatomic shoulder replacement is an effective treatment for many patients with advanced shoulder arthritis, it is not suitable for every shoulder condition. Successful outcomes rely on restoring the natural ball-and-socket joint while allowing the rotator cuff muscles to control and stabilise movement. In situations where these structures are significantly compromised, alternative treatment approaches may provide more reliable function and pain relief. Careful patient selection is essential to support safe recovery, long-term implant performance, and overall shoulder function.
Anatomic shoulder replacement relies on a functioning rotator cuff to control shoulder movement after surgery. If the rotator cuff tendons are severely torn, degenerated, or irreparable, the shoulder may remain weak or unstable following a conventional replacement.
In these cases, alternative procedures such as reverse shoulder replacement may sometimes be considered, as they use different biomechanics to keep the joint stable to compensate for rotator cuff deficiency.
Advanced arthritis or previous injury can sometimes result in substantial bone erosion, particularly affecting the shoulder socket (glenoid). When bone loss is severe, it may be difficult to safely secure the socket component or restore stable joint alignment using a standard anatomic implant.
In these cases reverse shoulder replacement often becomes the treatment of choice.
Shoulder replacement surgery is generally delayed or avoided in the presence of active infection within the joint or surrounding tissues.
A cut on the hand or arm on the same side will need to be healed over before a shoulder replacement.
Major dental work should be fully complete prior to surgery.
Similarly, poorly controlled medical conditions that increase surgical risk or impair healing may require optimisation before surgery can be safely considered. A notable example is poorly controlled diabetes.
Conditions that impair muscle function, nerve control, or coordination of shoulder movement may limit the effectiveness of anatomic shoulder replacement. In these circumstances, restoring the joint surfaces alone may not provide reliable functional improvement.
Some individuals involved in very heavy manual labour or repetitive high-impact activities may require careful discussion regarding implant durability and long-term expectations. Replacement prostheses wear out or fail in other ways more quickly in those who subject the components to higher loads. Replacement of the humeral head alone (hemiarthroplasty) may be considered in these circumstances.
Determining whether anatomic shoulder replacement is the most appropriate option requires detailed clinical evaluation and imaging assessment. Dr Richard Dallalana carefully considers rotator cuff integrity, bone quality, joint alignment, activity demands, and long-term functional goals when recommending treatment.
A thorough pre-operative assessment is essential to determine whether anatomic shoulder replacement is the most appropriate treatment and to plan surgery as safely and accurately as possible. Shoulder replacement surgery is highly individual, and careful evaluation helps ensure the procedure is tailored to your shoulder anatomy, symptoms, and functional goals.
Assessment begins with a comprehensive discussion about your shoulder symptoms, including:
A detailed clinical examination allows evaluation of shoulder movement, strength, stability, and overall joint function. Particular attention is given to:
Imaging plays a central role in confirming diagnosis, assessing arthritis severity, and planning implant positioning. Investigations commonly include:
Pre-operative evaluation also considers general health factors that influence surgical safety and recovery. This may include:
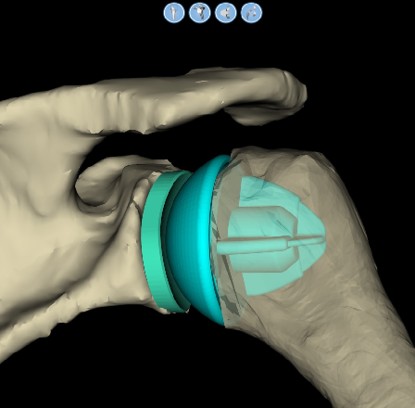
Using specialised planning software, the CT images are converted into a three-dimensional digital model of your shoulder. This allows Dr Dallalana to plan the procedure in detail before surgery takes place. Your operation is performed entirely on screen and important decisions are made ahead of time, often confirming whether an anatomic replacement is feasible or whether a different procedure such as a reverse shoulder replacement would be more suitable.
This planning will help with:
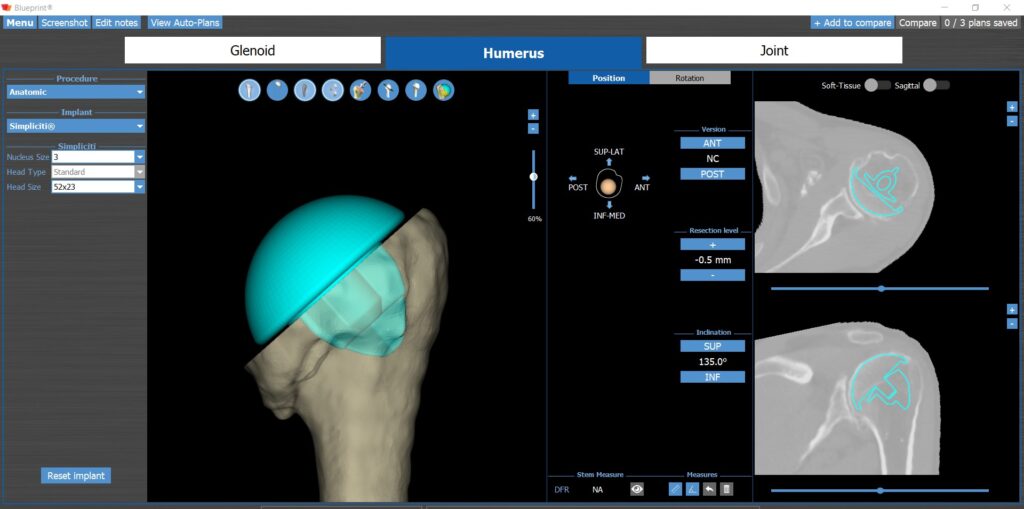
Personalised computer planning allows the surgical approach and implant positioning to be guided by your individual anatomy. Once the on-screen planning is complete, patient-specific (custom) instruments or guides are often manufactured to convert the pre-operative plan into the actual surgical outcome in the operating theatre.
These sterilised single-use guides are used during your procedure to guide perfect implantation of the shoulder prosthesis.
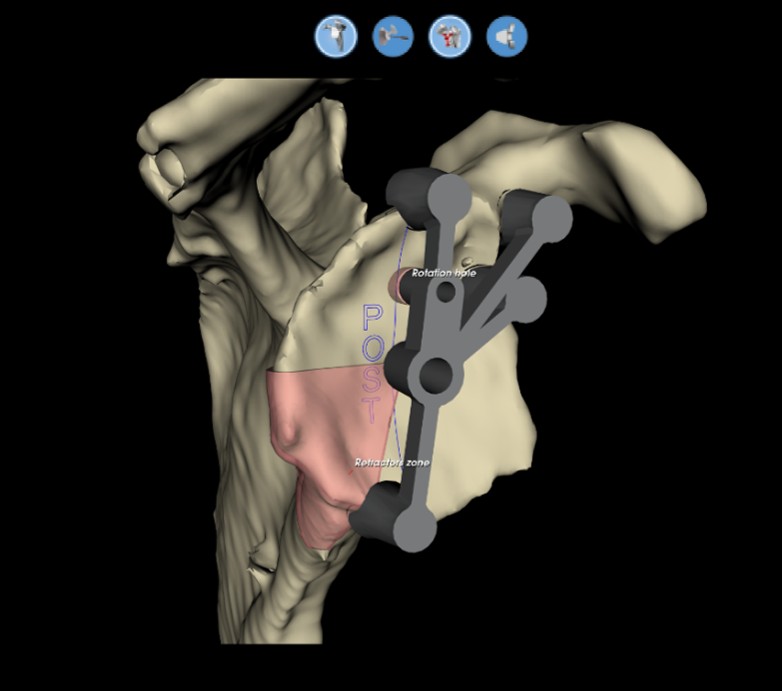
In addition to patient-specific instruments, accurate placement of components during surgery can also be carried out using navigation systems. These use camera systems connected to both the bone and to the surgical instruments during the operation to guide each carefully based on the computer planning performed prior.
Dr Dallalana will use this technology in some situations to add further accuracy, or when patient specific instruments are not available.

Advanced planning tools do not replace surgical expertise. Instead, they support decision-making and enhance precision when combined with careful clinical assessment and surgical experience. Dr Richard Dallalana integrates advanced imaging, personalised planning, and intraoperative judgement to optimise anatomic shoulder replacement surgery. During your consultation, he will explain how this planning process applies to your shoulder and how it supports surgical accuracy and long-term shoulder function.
Anatomic shoulder replacement surgery involves replacing the damaged joint surfaces with carefully designed prosthetic components that replicate the natural structure and movement of the shoulder. Modern shoulder replacement systems are developed using advanced biomaterials and engineering techniques to improve durability, fixation, and long-term performance.
Both a humeral and a glenoid component are required to replace both sides of the shoulder joint.
The humeral component replaces the damaged head of the upper arm bone (humerus). This implant is typically made from highly polished medical-grade metal designed to provide a smooth and durable joint surface. It is usually a chrome-cobalt alloy.
It is usual not to require a stem to go down the arm bone – ‘Stemless fixation’.
Stemless fixation of the humeral ball to the upper arm is almost always possible unless bone stock is very poor. This type of humeral replacement has been shown to have the best survival outcome figures in long term studies and is the prosthesis of choice used by Dr Dallalana.
It is a bone preserving approach compared to use of a longer stem down the arm
The glenoid component replaces the worn socket of the shoulder joint. This component is most commonly made from highly cross-linked polyethylene, a specialised medical-grade plastic designed to provide a low-friction, durable joint surface.
The glenoid component is secured to the shoulder blade using press-fit pegs, or a type of bone cement.
Anatomic shoulder replacement aims to replicate the natural ball-and-socket relationship of the shoulder joint. This allows the rotator cuff muscles to continue controlling movement and stabilising the joint. A natural feeling shoulder which looks and moves like a natural one is possible.
Modern shoulder anatomic replacement implants provide long-lasting function.
Implant survival depends on several factors including prosthesis type, your bone quality, implant positioning, age and activity levels after surgery.
Stemless anatomic implants have some of the best track records with regard to shoulder performance and length of survival of the prosthesis before repeat surgery is required.
Australian joint registry data shows that less than 5% of patients will require a repeat procedure within the first 10 years after implantation. Other international studies show that the vast majority of this type of implant will be functioning beyond 15 years. Modern design prostheses have not been followed for more than 20 years however the expectation is that once they reach 15 years without incident that they will continue to 20 or well beyond.
If the prosthesis wears out to the point of needing replacement it will have become painful and movement will be restricted. It may need to be revised to a new one, and this is usually to a reverse style prosthesis. Revision surgery is discussed in more detail on another page
During your consultation, Dr Dallalana will discuss implant options, expected performance, and factors that may influence long-term outcomes based on your specific shoulder condition.
Wound closure: Once the joint has been reconstructed and stability confirmed, the incision is closed with a buried dissolving suture and waterproof dressings are applied. Your arm is initially placed into a sling during early recovery.
The procedure typically takes approximately 1.5 to 2 hours, although surgical time can vary depending on the complexity of the shoulder condition.
On the day of surgery, you will arrive at the hospital at the time provided by the admissions team. Nursing staff will complete admission checks, confirm your medical history, medications, allergies, and fasting status, and help prepare you for theatre. You will also have an opportunity to ask any last-minute questions. Your shoulder will be marked to confirm the correct surgical site, which is a standard safety step performed before all procedures.
Before surgery, you will meet your anaesthetist, who will discuss your anaesthetic plan and pain management strategy. Anatomic shoulder replacement is typically performed under general anaesthesia, meaning you will be asleep throughout the procedure.
In many cases, a regional nerve block is also used. This involves numbing the nerves around the shoulder to help reduce pain after surgery. The nerve block can provide pain relief for several hours following the procedure and may reduce the need for strong pain medications during early recovery.
Once you are ready, you will be taken into the operating theatre where the surgical and anaesthetic teams perform final safety checks. These include confirming your identity, procedure, and surgical site as part of nationally recognised patient safety protocols.
You will then be positioned carefully to allow safe access to the shoulder while protecting pressure areas and maintaining comfort throughout surgery.
After surgery, you will be transferred to the recovery unit where nursing staff and anaesthetic teams monitor you as you wake from anaesthesia. Your arm will remain supported in a sling for initial protection.
Once the nerve block has worn off a sling will not be required while in hospital. Use of the arm for simple tasks such as eating and dressing are permitted, and further information about longer term use of a sling will be provided based on individual needs. As a general rule it will be used going forward for approximately 6 weeks only when walking for any length of time, and not while at rest or in bed.
Most patients remain in hospital for two nights, although this can vary depending on overall health and recovery progress.
During your hospital stay:
At time of discharge you will receive detailed guidance regarding sling use, exercises, medications, wound care, and follow-up appointments.
Prior to leaving hospital, your care team will ensure you feel confident managing your shoulder at home. Written rehabilitation instructions are provided to support your recovery.
If you have questions about the procedure or preparation for surgery, these can be discussed during your initial consultation with Dr Dallalana.

Pain management following anatomic shoulder replacement surgery is an important part of recovery and is carefully planned to support comfort, early movement, and safe rehabilitation. While some post-operative discomfort is expected, modern pain management strategies aim to keep pain well controlled and reduce reliance on strong medications where possible.
Dr Richard Dallalana works closely with the anaesthetic and hospital teams to ensure pain relief is tailored to your individual needs and medical history.
Anatomic shoulder replacement is performed under general anaesthesia and is often combined with a regional nerve block. The nerve block temporarily numbs the shoulder and upper arm, helping to reduce pain in the hours immediately following surgery.
The nerve block helps by:
As the nerve block wears off, other pain relief measures are gradually introduced to maintain comfort.
This approach prevents the experience of higher pain levels in the first few hours to 1 day following the procedure.
Use of the nerve block is commonplace, but not required for successful completion of the surgery, and you do not need to have this performed if you don’t wish to. This can be discussed with the anaesthetist on the day of surgery, or ahead of time if desired.
Post-operative pain is typically managed using a multimodal approach, meaning several methods are combined to improve pain control while limiting side effects.
This may include:
Using multiple pain control methods together often provides more effective relief than relying on a single medication alone.
Sleeping as upright as possible helps with pain relief.
NOT using a sling when in bed or at rest helps to control pain by allowing gentle movement at the shoulder and the freedom for it to rest in its own position of comfort, plus unrestricted use of the elbow and hand.
Pain levels usually improve gradually over the first few weeks following anatomic shoulder replacement surgery. Most patients notice that discomfort is greatest in the early recovery phase and steadily reduces as healing progresses and shoulder movement improves.
When you leave hospital, you will be provided with an initial supply of pain relief medications and clear instructions on how to take them safely.
During the weeks following surgery:
If you require additional pain medication once your initial supply has finished, prescriptions are generally provided by your GP, who can continue pain management in the community as required. Ongoing prescribing is not routinely provided through the surgical practice.
*Pain that worsens rather than improves, or pain associated with increasing redness, swelling, fever, or other concerning symptoms, should be reported for review.
Physiotherapy is an essential part of recovery after anatomic shoulder replacement. Early exercises are carefully guided and focus on gentle movement rather than strength.
Pain management supports rehabilitation by:
Your physiotherapy program is progressed in stages to balance healing with safe shoulder use.
Pain perception and medication tolerance vary between individuals. Factors such as previous shoulder pain, medication sensitivity, and other health conditions are considered when planning pain relief.
You should contact the practice or seek medical review if you experience:
Early assessment helps identify and address issues promptly.
Recovery after anatomic shoulder replacement surgery occurs gradually over several months. While every patient heals at a different rate, most recovery follows a predictable pattern as the shoulder adapts to the new joint and surrounding tissues regain strength and flexibility. The timeline below provides a general guide to what patients commonly experience following surgery. Your individual recovery plan may vary depending on surgical findings, overall health, and rehabilitation progress.
The early recovery phase focuses on protecting the shoulder while managing pain and swelling.
During this period, most patients can expect:
An appointment with Dr Dallalana is arranged at approximately 2 weeks from the surgery to remove the dressings and inspect the wound.
*Leave the dressings in place until this appointment. They are waterproof, and normal showering is permitted during this time..
Many patients can perform basic activities such as eating, dressing, typing, and light household tasks within the first two weeks.
During this stage, rehabilitation focuses on gradually restoring shoulder mobility while continuing to protect the repaired muscle (subscapularis).
You should notice:
Driving is not possible during this period due to limited strength and control of the arm
By this stage, healing tissues are generally stronger, allowing rehabilitation to include strengthening exercises and full movement range.
Typical milestones during this phase include:
Most patients begin noticing meaningful improvements in shoulder function and comfort during this stage.
Driving a vehicle is permitted
An Xray is performed to check on the prosthesis at the 3-month point, coupled with an appointment with Dr Dallalana in the office.
The focus during this phase shifts toward improving strength, endurance, and functional use of the arm.
Patients commonly experience:
Many patients are able to resume moderate physical activities such as gardening and non-contact sport such as golf during this period, depending on recovery progress.
Shoulder replacement recovery continues to evolve for up to twelve months following surgery.
During this later phase, patients may achieve:
While 90% of functional recovery occurs within the first six months, further improvements in strength and movement can continue for up to one year.
Final review with an Xray is undertaken at the 12 month point
Unless individually stated, all activities are permitted following anatomic replacement, including weights training, tennis, skiing and other sports.
Recovery after anatomic shoulder replacement varies between individuals. Factors that may influence recovery include:
The primary goals of anatomic shoulder replacement are to reduce pain, improve movement, and enhance shoulder function. Many patients experience substantial improvements in quality of life following surgery. Recovery is progressive, and patience is important as strength and mobility continue to improve over time. During your consultation and follow-up appointments, Dr Richard Dallalana will monitor your recovery progress and provide guidance tailored to your rehabilitation milestones and functional goals.
Many patients may return within approximately 2 to 4 weeks, provided they are comfortable and are not taking medications that affect concentration or alertness. If needed writing and keyboard work from home could commence within days.
Return to modified duties may be considered around 6 to 12 weeks following surgery, depending on strength and shoulder control.
Jobs requiring repetitive lifting, overhead activity, or sustained shoulder loading may require a longer recovery period. Return to full duties may take approximately 4 to 6 months or longer depending on speed of strength recovery.
Dr Richard Dallalana will provide guidance regarding safe work return timelines based on your occupation and rehabilitation progress.
Strength training is an important part of long-term shoulder function following joint replacement.
Lifelong modest weights training is permissible after anatomic shoulder replacement.
Exercises are initially introduced gradually to protect the joint and surrounding soft tissues.
Activities involving heavy lifting, repetitive overhead motion, or contact place increased stress on the replacement joint. Participation in these activities is considered on an individual basis but are usually permitted.
If bone quality is soft or the activity involves repeated extreme stress, then it may be ill-advised due to risk of implant wear or loosening.
Strength training is an important part of long-term shoulder function following joint replacement.
Lifelong modest weights training is permissible after anatomic shoulder replacement.
Exercises are initially introduced gradually to protect the joint and surrounding soft tissues.
Patients are typically guided to:
Your physiotherapist will provide tailored exercise programs designed to improve shoulder strength and endurance safely.
Self-directed weights training programs or under guidance of a personal trainer are suitable after 6 months following surgery.
Correspondence is routinely provided to your physiotherapist or trainer for guidance.
Anatomic shoulder replacement surgery is a well-established procedure that can significantly improve pain and function for appropriately selected patients. As with all surgical procedures, however, there are potential risks and complications that should be understood before proceeding with surgery.
During your consultation, Dr Richard Dallalana will discuss these risks in the context of your individual shoulder condition, overall health, and treatment goals to support informed decision-making.
The surgery is performed in a semi-recumbent position, approximately 30 degrees upright. Complications related to the general anaesthetic are very rare and relate in part to general health. Pre-surgical medical specialist assessment is arranged prior to shoulder joint replacement to assess medical health and optimise if needed.
Anaesthetic is slightly lighter if a regional nerve block is used. Specific risks related to the anaesthetic or the nerve block can be discussed with the anaesthetist ahead of time or on the day of surgery if desired.
Infection can occur early after surgery or, less commonly, at a later stage. Treatment depends on severity and may involve antibiotics or further surgery in selected cases.
This risk is approximately 1% of cases for anatomic shoulder replacement.
Some patients may experience ongoing stiffness after surgery. Rehabilitation and physiotherapy play an important role in optimising shoulder movement and preventing this. Severe stiffness limiting function is uncommon. Unexplained significant persistent stiffness can be a sign of low-grade infection.
Inability to reach fully behind the back (for e.g. to reach a bra) is occasionally noted if the muscles which allow this don’t recover adequate strength or internal joint scarring persists.
Although uncommon in anatomic shoulder replacement, instability may occur if soft tissue balance is affected by failure of the subscapularis repair to heal properly. This can happen if movement restrictions are not followed or the arm is used forcefully during early recovery.
In contrast to reverse shoulder replacement, actual dislocation of an anatomic replacement is very rare.
Anatomic shoulder replacement relies on a functioning rotator cuff. A healthy rotator cuff is a pre-requisite for this surgery in the first instance, but in a small group of people the rotator cuff can deteriorate in the years following the surgery and may affect shoulder strength and function. Occasionally this can lead to revision surgery, with most studies showing an incidence of this of around 1% within the first 10 years after surgery.
Injury to nearby nerves is very uncommon but may result in numbness, weakness, and potentially loss of adequate function. Rarely specific nerve treatment may be needed and is successful if a nerve injury is identified early.
A very rare complication which may require urgent attention during the surgery.
Bone fractures can occur following trauma after surgery, particularly in patients with reduced bone quality.
Specific implant designs reduce the risk of fracture such as the ‘stemless’ type shoulder replacement, or those with a very short type of stem on the humeral side.
The main consideration is loosening of the components from bone, and/or wearing out of the plastic socket resurfacing. Most modern implants and surgical techniques result in very low implant failure rates. High density polyethylene has improved significantly and is very reliable. The chrome-cobalt or ceramic humeral heads are polished to an extremely smooth finish.
Implant longevity varies between individuals and depends on factors such as activity levels and bone quality. Implants are chosen by Dr Dallalana which have modern materials and a proven track record of survival.
The incidence of component failure from wear or loosening requiring a revision within the first 10 years of surgery is <2%
Optimising health before surgery and following post-operative guidelines may help reduce complication risk.
For many patients, the potential benefits of anatomic shoulder replacement, including pain reduction and improved shoulder function, outweigh the risks of surgery when these are carefully considered and the surgery is planned and executed accurately. The decision to proceed with surgery is always individualised.
Dr Richard Dallalana will discuss expected outcomes, potential risks, and alternative treatment options to ensure the chosen management approach aligns with your condition and goals.
Anatomic shoulder replacement surgery is performed with the aim of reducing pain, improving shoulder movement, and restoring function for patients affected by advanced shoulder joint disease. Long-term outcomes vary between individuals and depend on several patient-specific and surgical factors.
Understanding what to expect over the months and years following surgery can help patients make informed decisions and engage actively in their recovery.
Most patients experience a gradual and sustained reduction in shoulder pain following anatomic shoulder replacement. Pain relief typically continues to improve over the first several months as healing progresses and shoulder movement becomes more comfortable.
While many patients report significant improvement compared to their pre-operative symptoms, occasional discomfort with heavy or repetitive use may still occur, particularly in the early years after surgery.
Improvements in shoulder movement and strength occur progressively with rehabilitation. Over time, most patients regain the ability to perform activities such as:
Final shoulder movement is usually at 12 months from surgery and varies depending on pre-operative stiffness, rotator cuff health, and adherence to rehabilitation programs.
Anatomic shoulder replacement compared to other prosthetic types has the highest average movement range at the end of the full recovery period, and often approximates a normal shoulder.
Implant longevity varies between individuals and depends on age, activity levels and bone quality.
Implants are chosen by Dr Dallalana which have modern materials and a proven track record of survival. The incidence of component failure from wear or loosening requiring a revision within the first 10 years of surgery is <2%. The vast majority will last for 15 to 20 years barring any specific complication.
Ongoing care after shoulder replacement may include:
Whilst uncommon, some patients may require further treatment, which may include repeat surgery, due to:
If revision surgery is required, early assessment helps guide appropriate management.
Dr Richard Dallalana works closely with patients to set realistic expectations, guide activity choices, and support long-term shoulder health following anatomic shoulder replacement surgery.
Anatomic and reverse shoulder replacement procedures are primarily designed for different shoulder conditions. Neither procedure is considered universally better. Each has advantages and disadvantages, and this is a key discussion at initial consultation. Careful assessment is required to determine which procedure may be most suitable for each patient. 3D computer modelling is used by Dr Dallalana to assist with this determination in all cases.
Non-surgical treatments are almost always utilised before considering joint replacement and may include:
These treatments aim to manage symptoms but do not reverse advanced joint degeneration. Suitability depends on symptom severity and level of arthritis.
Some patients choose to delay surgery while managing symptoms with non-operative treatment. In certain situations, progressive joint damage, stiffness, or muscle changes may influence future treatment options.
It is sometimes safe to delay surgery, particularly when young, and at other times it is best to undergo replacement before advanced changes such as bone erosion occur limiting options. Regular review allows symptoms, function, and imaging findings to be monitored so that treatment decisions can be adjusted when needed.
Some discomfort is expected after surgery, particularly in the early stages. Pain is managed using a structured, multimodal approach and typically improves steadily as healing progresses. Pain control in the first day is greatly assisted by a nerve block which will be offered. Beyond the first day tablets alone are adequate to control pain, and strong medication such as opiates like endone or palexia are not needed for more than a few days. Pain is well controlled by the second week after surgery.
Most patients are surprised at how quickly pain settles and this relates somewhat to the painful arthritic bone being removed during the surgery.
Hospital stay is usually short: 2 days in 95% of cases.
Discharge planning focuses on ensuring you feel safe, comfortable, and supported before returning home.
Inpatient rehabilitation is required on some occasions particularly if there are no supports around the home and this is arranged during your hospital stay.
Physiotherapy begins day 1 after surgery, initially focusing on gentle, protected movement.
You will be seen by the physiotherapy team in the hospital and shown how to do the exercises, and a printed instruction sheet is provided to keep these going at home. These instructions will cover the first 6 weeks, and beyond that exercise progression and finalising all aspects of your rehabilitation will be coordinated by a community physio. This can be with your own chosen practitioner, or one recommended by Dr Dallalana.
Driving is generally resumed once the sling is no longer required and you can safely control the vehicle. This varies between individuals but is at the 6 week point in most cases.
Return-to-work timing depends on the physical demands of your job. Sedentary roles may be possible earlier, while physically demanding work often requires a longer recovery period and a graded return. Office work can commence within days if needed and the sling can be removed to use a keyboard.
In most cases movement is very close to that of a normal shoulder, but not at 100%. Pre-operative stiffness, muscle health, and adherence to rehabilitation all influence outcomes. It is rare to not have a high range of motion or to have a limitation enough to impair activities.
Almost everything is permitted after anatomic shoulder replacement.
Some very high-load or dangerous activities may be discouraged to help protect the joint over time. Guidance on allowed activities is tailored to your shoulder, implant configuration, and lifestyle goals.
Barring any major complication, a meaningful improvement in pain and shoulder function following surgery is expected. Specific outcomes vary depending on individual shoulder condition, rotator cuff health, rehabilitation participation, and overall health factors.
During consultation, Dr Richard Dallalana discusses expected benefits and limitations of surgery based on individual clinical findings.
Shoulder replacement surgery is commonly performed to improve comfort, movement, and ability to perform daily activities when shoulder arthritis or joint damage significantly affects function.
Modern shoulder replacement implants are designed for long-term use. Longevity varies depending on factors such as implant positioning, bone quality, activity level, and overall shoulder health.
It is rare to require repeat surgery within 10 years (<4%), and most will last for 15 to 20 years.
Most people do not require additional surgery however, as with any joint replacement, wear with time may require the procedure to be repeated. The younger one is at the time of surgery, the more likely a repeat procedure will be needed.
Further surgery may be required in the unlikely event of a complication such as a fracture or infection.
Age alone does not determine suitability. Occasionally it is the best option even for very young patients. Decisions are based on severity of symptoms, joint condition and potential for deterioration in the future, activity level, and response to non-surgical treatment. These factors are assessed individually.
The key potential risks are infection, stiffness, implant wear or loosening, rotator cuff weakness or tearing. These and other risks are discussed in detail before surgery so you can make an informed decision.
Patients commonly ask me about:
These concerns are discussed in detail during consultation to help you feel informed and supported when making treatment decisions.
The cost of shoulder replacement surgery varies according to hospital and surgeon fees, prosthesis costs, anaesthetic and assistant fees, imaging requirements, and post-operative care. Out-of-pocket expenses can differ between patients depending on private health insurance coverage and individual policy inclusions.
All patients undergoing surgery with Dr Dallalana are provided with detailed cost information prior to surgery to help support informed financial planning.
Yes, shoulder replacement surgery is possible without private health insurance through self-funded (self-pay) arrangements in the private sector.
Dr Dallalana does not currently operate in public hospitals.
Self-funded surgery involves paying directly for hospital, prosthesis, anaesthetic, surgical and assistant costs.
A detailed quote outlining all of these expected costs and anticipated return from Medicare is provided to help you make an informed decision.
Choosing a shoulder surgeon is an important decision and should consider:
Consultation allows patients to ask questions, understand available treatment options, and determine whether they feel comfortable with their surgical care plan.
Most patients benefit from assistance at home during the early recovery period, particularly within the first 6 weeks. Support may include help with:
Planning home support before surgery may help recovery progress more smoothly.
Most people do not need specific help with dressing and basic self-care.
Patients are generally advised to bring:
Specific instructions are provided before hospital admission.
Shoulder replacement implants contain metal components that may occasionally activate security scanners. Patients can inform airport security that they have a joint replacement if required. Documentation can be provided if travel is planned soon after surgery.
Timing if travel depends on pain levels and degree of assistance by others. There is no medical reason not to travel by plane, and there is no additional risk of DVT (blood clots in the legs) following shoulder surgery, in contrast to surgery on the legs.
Travel plans should be discussed ahead of time to ensure safety and that key steps in the rehabilitation will not be missed.
Message sent