

Shoulder dislocation and instability occur when the ball of the shoulder joint (the humeral head) moves partially or completely out of the socket (the glenoid). This can result in pain, weakness, loss of confidence in the shoulder, and an increased risk of further injury if not appropriately managed.
Because the shoulder allows a large range of motion and has relatively little inherent bony stability, it is particularly vulnerable to instability following trauma such as a sports injury, or repetitive stress.
The shoulder socket is naturally shallow and is often compared to a golf tee, with the ball of the shoulder joint sitting on top. There is little by way of bone structure to keep the ball in place.
Unlike joints such as the hip, shoulder stability relies heavily on soft tissue structures rather than bone.
The rotator cuff muscles which surround the joint provide an additional layer of stabilisation
When the glenoid labrum and/or ligaments are torn or stretched, the shoulder may no longer remain centred during movement, leading to instability.
Anterior shoulder dislocation is the most common type, where the humeral head moves forward out of the socket.
Posterior instability is when the humeral head shifts backwards. It is less common, and symptoms are more often pain with lifting or overhead use and a feeling of slipping in the shoulder rather than full dislocations. It may evade diagnosis and mimic impingement and other types of shoulder problems. There may not be a history of a specific injury.
Multi-directional instability (MDI) occurs due to loose ligaments of the shoulder an individual is born with. The labrum is not usually torn. The shoulder moves in any direction. The looseness may not cause any issues until an injury alters shoulder muscle balance following which pain or repeated dislocations and feelings of subluxation start to occur.
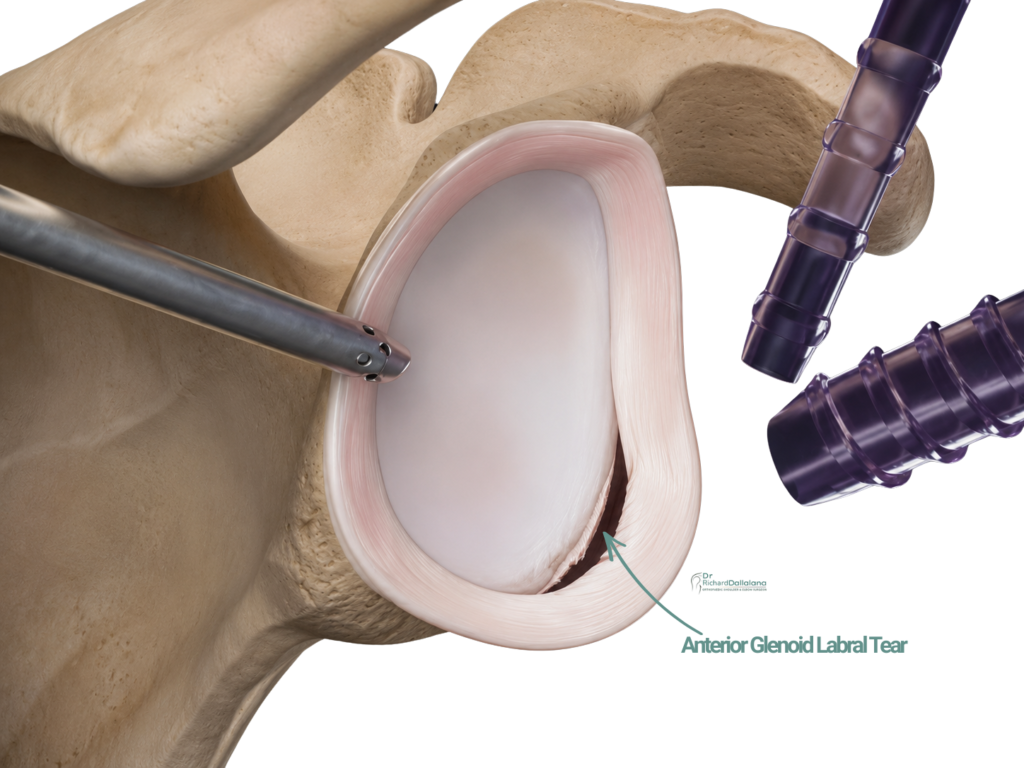
Labral and Soft Tissue Injury (Bankart Lesions): For a shoulder to dislocate, injury to the labrum and joint capsule almost always occurs. In anterior dislocations, this typically results in a tear of the front portion of the labrum, known as a Bankart lesion. This injury compromises the shoulder’s ability to remain centred during movement and significantly increases the risk of further dislocations if left untreated.
Bone Injury associated with Shoulder Instability: With repeated or severe dislocation, injury to the bone may also occur.
Common examples include:
In active people, particularly those involved in contact or overhead sports, shoulder instability carries a high risk of recurrence (repeated dislocations).
Risk factors include:
In young athletes the risk of re-dislocation after a single traumatic dislocation is very high without surgical stabilisation. Repeated instability episodes expose the joint cartilage to shear forces, increasing the risk of early shoulder arthritis over time.
In patients over the age of 40, recurrent instability is often less common. Instead, shoulder dislocation in this age group is more frequently associated with acute rotator cuff tears. Persistent pain and weakness following reduction of a dislocation may indicate rotator cuff injury. In these cases, imaging such as an MRI is commonly recommended to assess tendon integrity and guide management.
Surgical stabilisation may be considered when instability is recurrent, functionally limiting, or associated with structural injury such as a labral tear.
Anterior labral tears are themselves pain free but often need to be repaired to prevent recurrent dislocation
Posterior labral tears can be painful, and repair is often needed as much to control pain as it is for prevention of instability
The younger and the more active an individual, the more likely the shoulder will dislocate repeatedly if a labral tear is present.
Surgical stabilisation, usually an arthroscopic labral repair, is strongly advised in young athletic people after a single dislocation event when the labrum is torn, to prevent repeated dislocations for which the chance is very high.
Arthroscopic Shoulder Stabilisation: For patients with isolated soft tissue injury and minimal bone loss, surgery involves repair of the labrum and ligaments /capsule using minimally invasive techniques.
Bone Reconstruction Procedures: When instability is associated with significant bone loss or when lifestyle will result in repeated high energy injuries, procedures such as the Latarjet procedure or other bone reconstruction techniques may be recommended to restore stability.
In some cases of posterior instability the socket of the shoulder (glenoid) may be angled backward as a natural variant or as a result of numerous subluxation events, and re-shaping procedures to the bone may be advised
Dr Richard Dallalana provides specialist assessment and management of shoulder impingement and bursitis, guiding treatment decisions based on symptoms, imaging findings, and functional needs. A thorough assessment can help clarify the diagnosis and guide appropriate management.
Message sent