

The underlying cause of shoulder arthritis varies from person to person. In most cases, a clear cause is never identified, and this is referred to traditionally as primary arthritis. When a cause can be identified, it is better described as secondary arthritis.
Primary shoulder arthritis develops without a clear prior injury or event. Factors that may, however, increase the likelihood of developing primary arthritis include:
This is usually referred to as primary osteoarthritis.
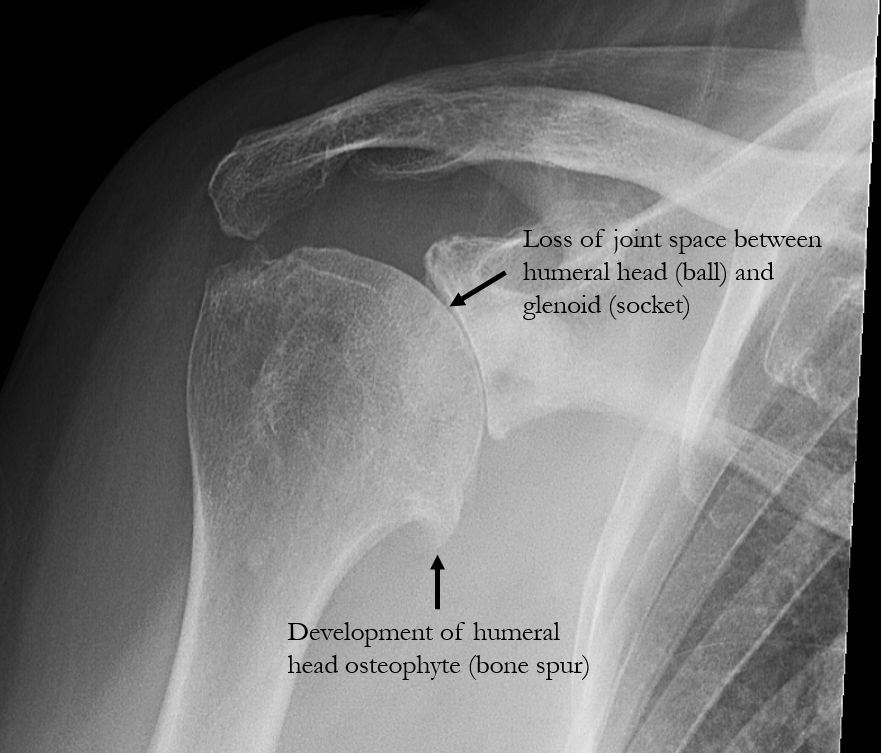
As the cartilage wears away, the joint surfaces become rough and irregular. Shoulder movement then creates friction, leading to inflammation within the joint, which is the primary source of pain in shoulder arthritis. As arthritis advances further, continued cartilage loss leads to narrowing of the joint space. Eventually the bones start to rub together, this is often described as “bone-on-bone” arthritis.
In severe cases, usually when the arthritis has been present for many years, the bone itself starts to erode away, usually on the socket side of the joint (glenoid). Treatment options become more limited.
Early in the condition, pain may occur only with specific movements or heavier activity. As arthritis progresses, pain may be present during routine daily activities and at rest. Weakness and functional limitation worsen with duration of the arthritis.
The condition is permanent and generally progresses with time. Heavy physical demands on the shoulder may accelerate the arthritis while modest activity is not known to worsen the condition.
If shoulder pain, stiffness, or reduced movement is persistent or progressively worsening, specialist assessment can help determine whether arthritis is present and whether joint replacement surgery may be appropriate. Dr Richard Dallalana performs a comprehensive evaluation to identify the cause of symptoms, assess joint function, and guide treatment recommendations based on individual needs and functional goals.
Diagnosis involves a combination of clinical assessment and imaging, including:
Treatment options may include:
Inflammatory arthritis can be managed with a range of medication, usually prescribed by a rheumatologist.
If non-surgical treatments no longer provide adequate relief, surgery may be considered based on symptoms, imaging findings, age, activity level, and rotator cuff function.
Arthroscopic surgery does not restore cartilage or stop arthritis progression, but it may improve pain and movement in selected cases.
For more advanced shoulder arthritis, joint replacement surgery may be the most appropriate treatment. This is usually when non-operative measures no longer provide sufficient relief. Occasionally replacement may be required relatively early after the diagnosis is made if bone erosion is severe or use of the arm is very severely limited.
Shoulder replacement involves resurfacing the damaged joint surfaces with prosthetic components designed to reduce pain and improve function. The most suitable type of replacement depends on age, bone quality, rotator cuff health, and individual functional requirements.
Dr Richard Dallalana will carefully assess your shoulder and discuss which option is most appropriate for your condition, including likelihood of success and expected survival of the prosthesis used.
Dr Dallalana provides specialised assessment of shoulder arthritis to determine the most suitable management approach based on individual needs.
Message sent