

Revision shoulder replacement is a procedure that may be considered when a previous shoulder replacement is no longer functioning as expected. This can occur for several reasons, including implant wear, loosening, instability, infection, or changes in the surrounding bone and soft tissues over time.
Revision surgery is typically more complex than primary shoulder replacement and requires careful assessment and detailed planning to understand the cause of symptoms and determine the most appropriate treatment approach.
Revision shoulder replacement is a procedure used to treat problems that can develop after a previous shoulder replacement. This involves removing and replacing some or all of the existing implanted components and addressing any changes in the surrounding bone and soft tissues.
Over time, a shoulder replacement may no longer function as expected. This can occur due to wear of the implant, loosening, instability, infection, or changes in the rotator cuff or bone. When this happens, revision surgery may be considered to improve comfort and restore function.
Revision procedures are often more complex than the initial (primary) shoulder replacement. This is due to factors such as bone loss, scar tissue, muscle weakness, or well-fixed previous implants which need to be removed.
Depending on the underlying issue, revision surgery may involve:
These symptoms can develop gradually or, in some cases, occur more suddenly.
Revision shoulder replacement may be considered when a previous shoulder replacement is no longer providing adequate pain relief or function, has dislocated or loosened, or become infected.
The condition of the bone and soft tissues is an important consideration, as this can influence both the type of revision required and expected outcomes. General health, activity level, and recovery goals are also taken into account when considering whether revision surgery may be appropriate.
Not all patients with adverse symptoms after shoulder replacement will require revision surgery.
In some cases, non-surgical management or monitoring alone may be more suitable, depending on the nature and severity of the problem.
Careful assessment and detailed planning are essential before revision shoulder replacement. The aim is to identify the cause of your symptoms and understand the condition of the implant, bone, and surrounding soft tissues.
Your shoulder is assessed to understand how it is functioning and where the main issues are.
This includes evaluating:
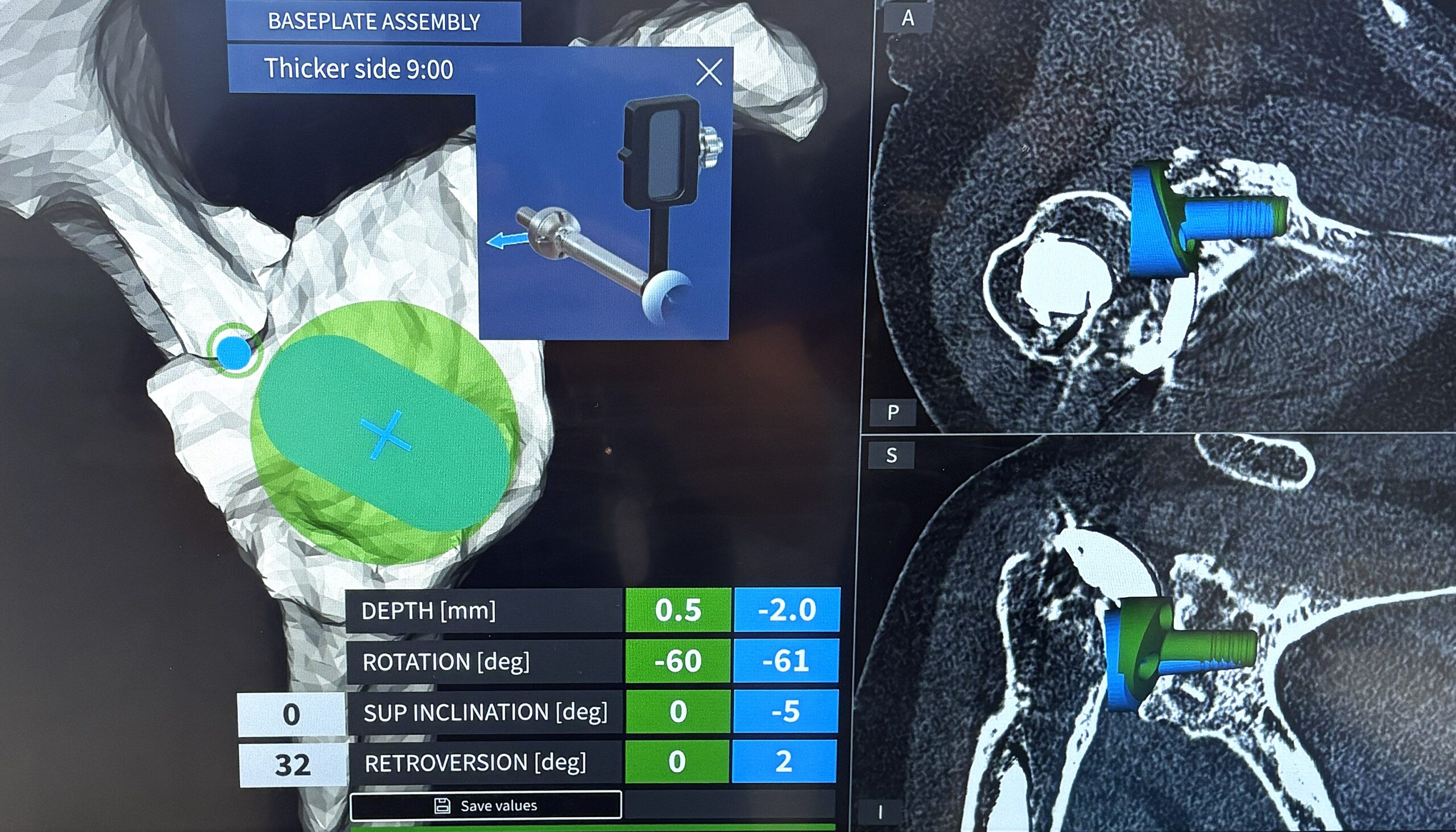
Imaging is used to assess both the implant and the underlying bone and soft tissues.
This may include:
Revision shoulder replacement is tailored to the underlying problem and the condition of the implant, bone, and surrounding soft tissues. The procedure may involve removing and replacing some or all of the existing components and reconstructing the joint to restore stability and function.
Removal of existing well-fixed metallic components can be difficult and sometimes involves creating a controlled split in bone, for example in the humeral shaft to remove the stem part of an existing replacement.
Bone loss is frequently encountered and requires bone grafting or other techniques to rectify.
Existing parts of the shoulder replacement may be removed and replaced with new components. Occasionally, a worn part can be exchanged for a new one with a relatively simple procedure.
An anatomic shoulder replacement may be revised to a reverse shoulder replacement if it has worn out, come loose, or the rotator cuff has torn. A torn rotator cuff cannot be repaired like it can be in a normal shoulder when a shoulder replacement has been performed.
A failed anatomic replacement can only very rarely be replaced with another of the same, and most often is revised to a reverse replacement.
This is usually revised to another reverse replacement with restoration of lost bone stock on the glenoid side, humeral side, or both. It is more complex than revising an anatomic replacement to a reverse. In most cases, the ball (glenosphere) has loosened from bone while the stem has remained sound. A new one can usually be implanted with bone grafting behind it on the socket.
In some cases, it is not possible to reimplant a reverse replacement, and a salvage option is to convert it to a hemiarthroplasty (half replacement). This is where a ball is replaced on the top of the humeral stem only and moves on the residual bone left in the socket. Pain relief is usually reasonable, but movement is generally limited.
Bone loss around the joint during revision surgery is commonly encountered and may be addressed using specialised implants, metallic augments, or bone grafting techniques to support implant fixation. Revision surgery often involves replacing lost bone on the glenoid side of the shoulder. This can be harvested from the hip (iliac crest) through a 3 cm incision during the same procedure. Donated bone or artificial bone substitutes can be used in some circumstances, usually when less structural demand is placed on the graft.
If the defect is too large, a custom-made component made from printed titanium can be created to any size and shape to fill the defect.
Techniques may be used to improve joint stability where instability or dislocation has occurred. This is usually in the context of reverse replacement and initially involves swapping out the existing plastic liner for a thicker one, and exchanging the ball (glenosphere) for a larger one. This is a relatively simple type of revision with a quick recovery.
In cases of infection, revision may involve staged procedures, including removal of the implant, treatment of infection, and later re-implantation. A temporary spacer filled with antibiotics may need to be left in the shoulder for a period of months between removal of the original prosthesis and implantation of a new one once the infection has been fully treated.
Revision surgery is more complex than primary shoulder replacement. The duration of surgery is longer, typically 2 to 3 hours, however up to 5 hours in very difficult cases. Complication rates are higher.
Recovery after revision shoulder replacement is typically slower and more gradual than after primary surgery.
Your arm will usually be supported in a sling for several weeks, usually 6, to protect the repair. Gentle, guided movement begins early, with exercises focused on maintaining basic mobility while allowing healing.
Physiotherapy plays an important role and progresses in stages, depending on the type of revision performed.
The pace of progression varies between individuals and depends on factors such as bone quality, soft tissue condition, and the complexity of the surgery.
An individualised rehabilitation plan will be provided.
Most patients are able to return to light daily activities within the first few weeks, with gradual improvement over time.
As a general guide:
Full recovery can take up to 12 months.
The aim of revision surgery is to improve pain and function. Outcomes can vary depending on the reason for revision and the condition of the shoulder. In many cases, meaningful improvement in comfort and function can be achieved, although movement and strength may not return to the same level as a primary shoulder replacement.
Your rehabilitation plan will be tailored to your procedure.
Revision shoulder replacement is a well-established procedure however, it is more complex than primary shoulder replacement and requires careful surgical planning and technique. As with all surgery, there are potential risks and complications that should be understood before proceeding.
Steps are taken before, during, and after surgery to help reduce these risks.
The likelihood of these risks varies depending on the reason for revision, bone quality, and overall health.
The aim of revision shoulder replacement is to improve pain and restore function.
Outcomes can vary depending on:
Many patients experience meaningful improvement in comfort and daily function. Outcomes may not be the same as a primary shoulder replacement, particularly in more complex cases.
The decision to proceed with revision surgery is individual. It involves weighing the potential benefits of improved pain and function against the risks of surgery. Revision shoulder replacement is a more complex procedure, and careful assessment and planning are important when considering treatment options. As part of this process, patients may also wish to consider factors such as a surgeon’s training, experience in managing complex shoulder conditions, communication style, and the level of support provided throughout the surgical journey.
Dr Richard Dallalana will discuss these considerations with you in the context of your specific shoulder condition, previous surgery, and treatment goals to support informed decision-making. He has particular expertise in revision surgery and complex reconstruction techniques.
A shoulder replacement may require revision if it no longer functions as expected. Common reasons include implant loosening or wear, infection, instability, rotator cuff failure.
Yes. Revision surgery is generally more complex than primary shoulder replacement because it involves working around existing implants, altered anatomy and scar tissue, and, in many cases, bone loss or soft tissue damage.
This depends on the problem. In some cases, only part of the implant is revised, while in others, all components are removed and replaced.
Yes. This is a common approach, particularly when the rotator cuff is no longer functioning adequately. The most suitable option depends on your individual shoulder condition.
Revision procedures often take longer than primary surgery due to their complexity. The exact duration depends on the nature of the revision and what needs to be addressed. It is typically 2 to 3 hours but may be up to 5.
Hospital stay is usually from 2 to 3 days, depending on the complexity of the surgery and your recovery.
Recovery is often more gradual than after primary shoulder replacement. The timeline depends on the type of revision performed and the condition of the bone and soft tissues.
The aim is to improve pain and function. While many patients achieve meaningful improvement, movement may not return to the same level as a primary shoulder replacement.
Risks may include infection, instability, nerve injury, fracture, stiffness, and implant-related complications. These risks vary depending on individual factors and are discussed prior to surgery.
Longevity varies depending on factors such as implant type, bone quality, and activity level. Average longevity is less than that of primary replacement. Complication rates described above are higher and these can lead to repeat surgeries or re-revision.
Most patients can return to daily activities with improvement in comfort and function. Higher-demand activities may need to be modified depending on the type of reconstruction. High impact activities are not usually recommended.
In some cases, non-surgical management such as physiotherapy, activity modification, or medication may be considered. The most appropriate approach depends on your symptoms and underlying condition. If bone is wearing out due to a worn out or loose prosthesis, then it is recommended to undergo revision surgery before it becomes very difficult or impossible to do so, even if symptoms are mild. Regular monitoring is very important.
Support at home is often helpful in the early recovery period, particularly for tasks such as cooking, cleaning, and transport.
This is based on a combination of symptoms, imaging findings, and overall shoulder function. All treatment options are considered to determine the most appropriate approach for your situation.
Message sent